2026: Volume 5, Issue 1
Current Issue
 Abstract
Abstract  PDF
PDFBeyond the Cough: Incidentally Detected Complete Atrioventricular Block in a Stable Child With URTI Symptoms
Altagy Sameer Albahlool1*, Yasmeen Abdullah Al-Harmali2Altagy Sameer Albahlool1*, Yasmeen Abdullah Al-Harmali2
1Emergency Physician, Medical City for Military and Security Services, Muscat, Sultanate of Oman
2Emergency Senior Specialist, Medical City for Military and Security Services, Muscat, Sultanate of Oman
*Corresponding author: Dr. Altagy Sameer Albahlool, Emergency Physician, Medical City for Military and Security Services, Muscat, Sultanate of Oman, Phone: +968 92169442, E-mail: [email protected]
ABSTRACT
Incidental severe bradycardia in children requires structured evaluation. A 4-year-10-month-old boy presenting with upper respiratory tract infection (URTI) symptoms was found to have complete atrioventricular (AV) block. Holter monitoring demonstrated persistent AV block (average heart rate 44 bpm, minimum 34 bpm). Echocardiography revealed structurally normal cardiac anatomy with preserved systolic function (EF 66%, FS 36%). After systematic exclusion of reversible causes, a single-chamber permanent pacemaker was implanted. This case emphasizes structured diagnostic reasoning and cautious interpretation of pediatric conduction disorders.
Keywords: Bradycardia, Echocardiography, Upper Respiratory Tract Infection, Atrioventricular
Received Date: January 02, 2026 Published Date: March 10, 2026
Citation: Albahlool AS, et al. (2026). Beyond the Cough: Incidentally Detected Complete Atrioventricular Block in a Stable Child With URTI Symptoms. Cases. 5(1):26.
Copyright: Albahlool AS, et al. © (2026).
INTRODUCTION
Persistent bradycardia in children is most commonly secondary to reversible causes such as hypoxia, metabolic disturbances, infection, or increased vagal tone. However, complete atrioventricular block beyond infancy is uncommon and requires careful evaluation to differentiate between congenital, idiopathic, and acquired etiologies. Incidental detection during evaluation for unrelated symptoms presents a diagnostic challenge [1-5].
CASE PRESENTATION
A 4-year-10-month-old previously healthy boy presented with four days of fever, cough, and rhinorrhea. During evaluation for URTI symptoms, incidental bradycardia (40–48 bpm) was detected. The patient was alert, well-perfused, and hemodynamically stable (BP 100/65 mmHg, SpO? 99% on room air). There were no signs of heart failure.
Electrocardiographic Findings
Initial 12-lead ECG demonstrated complete atrioventricular dissociation with independent atrial and ventricular activity. A narrow QRS escape rhythm was observed at approximately 44 bpm.
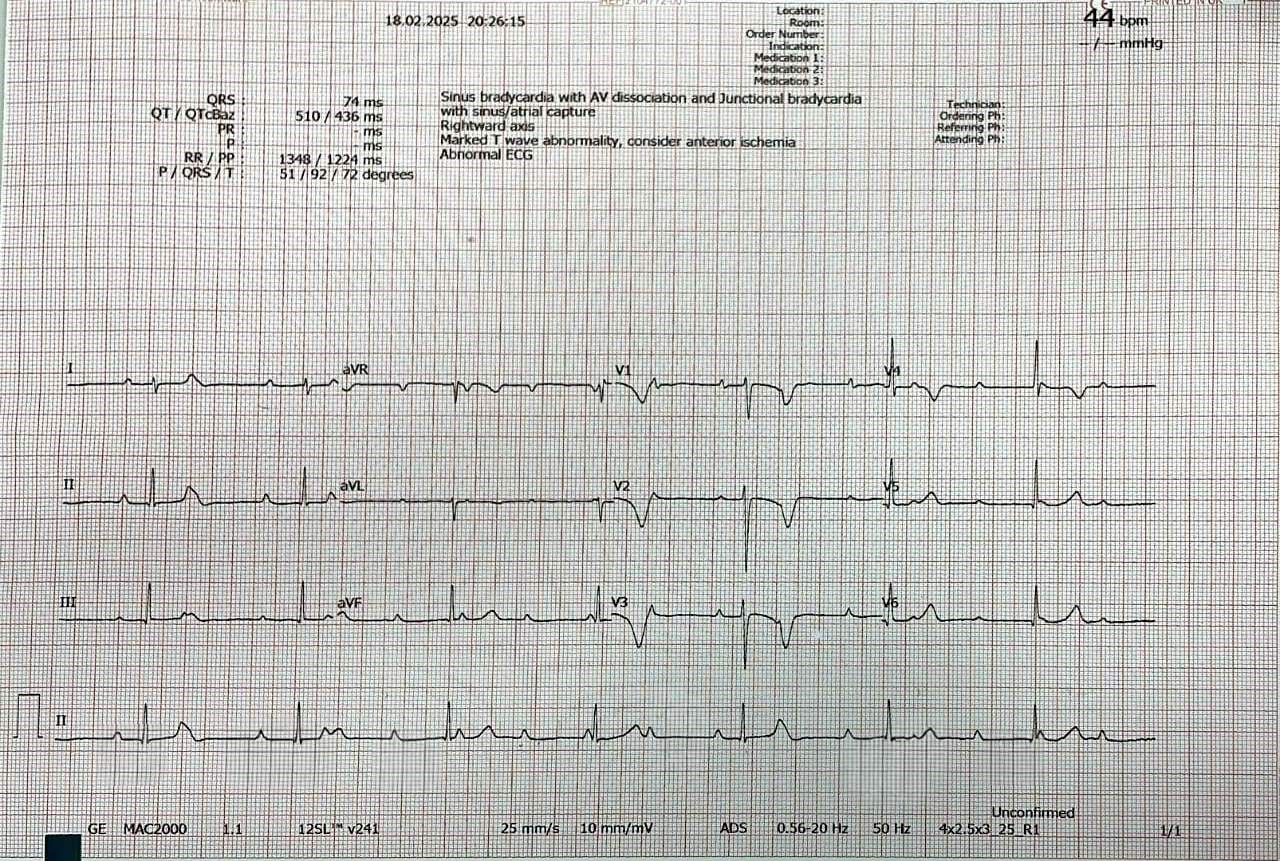
Figure 1: Pre-implant ECG demonstrating complete AV block with narrow QRS escape rhythm.
The narrow QRS morphology is suggestive of a junctional escape focus; however, precise anatomical localization cannot be determined from surface ECG alone.
Holter Monitoring
Twenty-four-hour Holter monitoring documented persistent complete AV block throughout recording. Total QRS complexes were 52,748. Average heart rate was 44 bpm, with a minimum of 34 bpm and maximum of 70 bpm. No significant pauses were recorded. Ventricular ectopic activity and short idioventricular rhythm episodes were observed.
Management and Post-Implant Evaluation
Given persistent severe bradycardia and objective Holter findings, single-chamber permanent pacemaker implantation was performed. Post-procedure heart rate was maintained between 70–90 bpm with stable hemodynamics.
Post-implant ECG confirmed appropriate pacing capture and ventricular activation pattern.
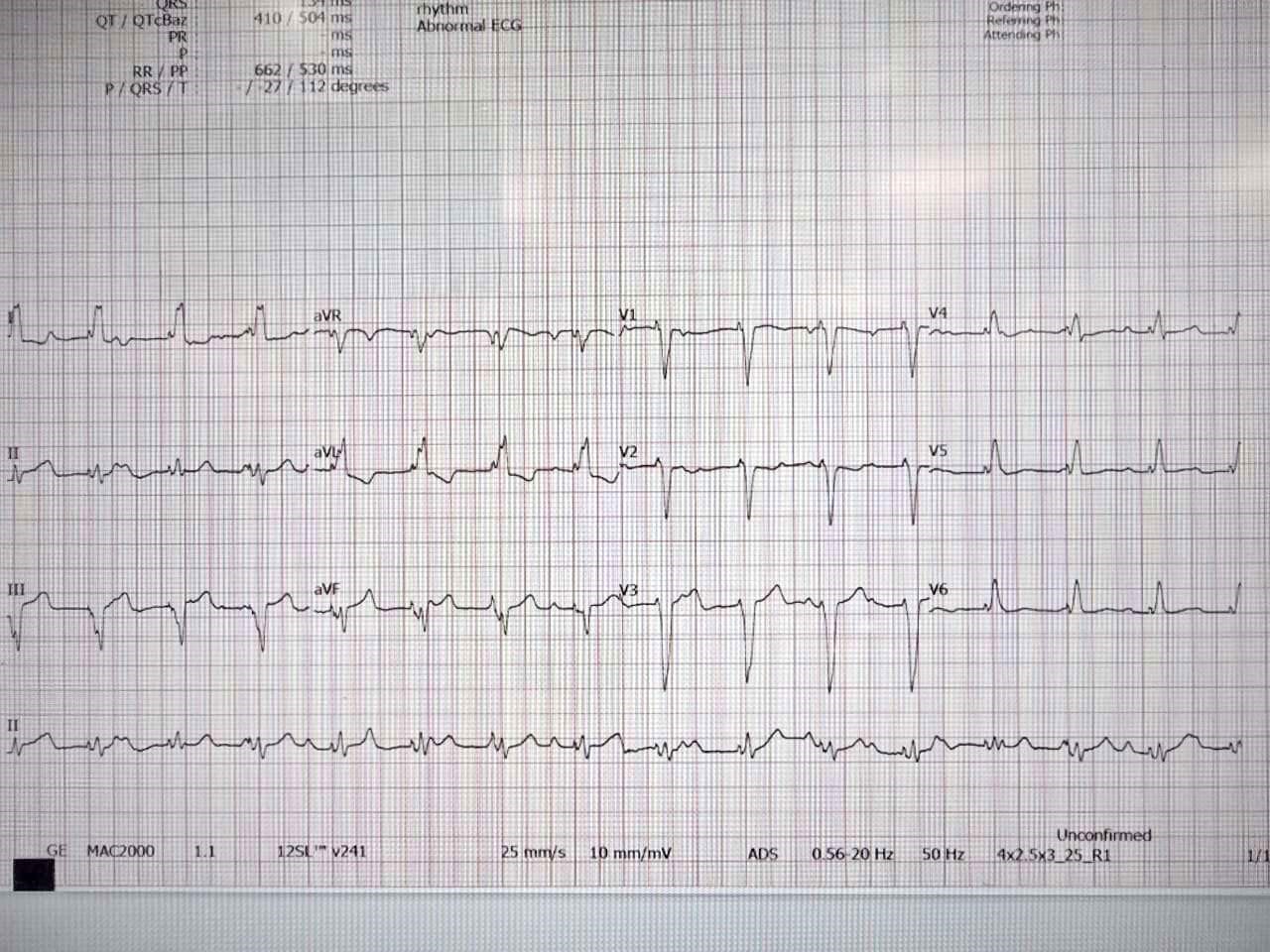
Figure 2: Post-implant ECG demonstrating appropriate ventricular pacing capture.
Post-procedural chest radiography confirmed appropriate pacemaker lead position and generator placement.
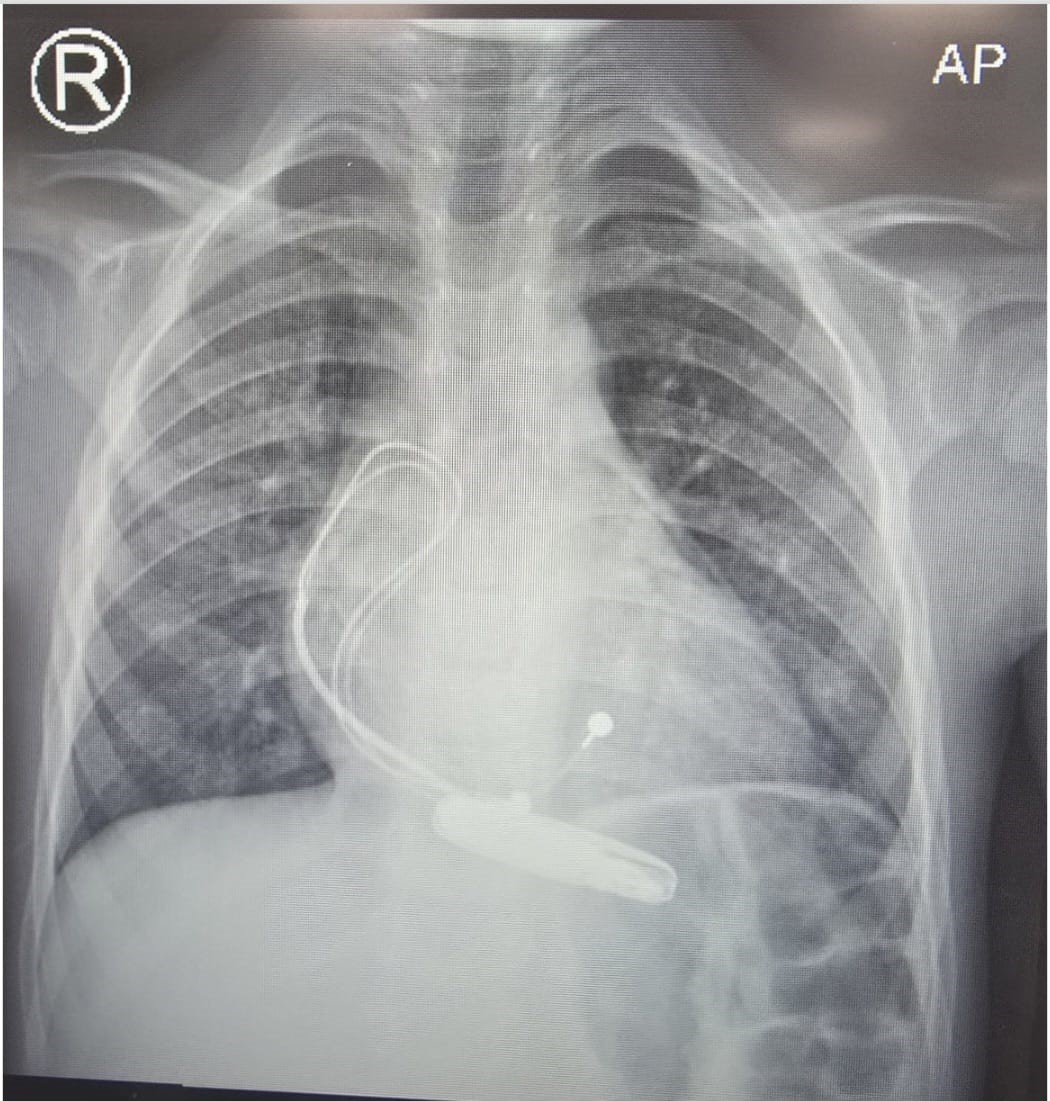
Figure 3: Post-pacemaker chest X-ray (AP view) showing appropriate lead positioning without complications.
DISCUSSION
This case highlights the importance of structured evaluation of pediatric bradycardia. Although the narrow QRS escape rhythm is suggestive of a junctional origin, anatomical localization cannot be confirmed without electrophysiological study. Systematic exclusion of reversible causes is essential before assigning etiology. Objective documentation of severe bradycardia justified pacemaker implantation despite clinical stability.
CONCLUSION
Complete AV block may be incidentally identified during evaluation for common pediatric conditions. Persistent severe bradycardia warrants structured investigation and objective risk assessment. Cautious diagnostic interpretation and evidence-based management are essential.
STATEMENTS
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Consent for Publication
Written informed consent for publication was obtained from the patient’s mother.
REFERENCES
- Shah MJ, Silka MJ, Silva JNA, Balaji S, Beach CM, Benjamin MN, et al. (2021). 2021 PACES expert consensus statement on the indications and management of cardiovascular implantable electronic devices in pediatric patients. Cardiology in the Young. 2021;31(11):1738-1769.
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) With the special contribution of the European Heart Rhythm Association (EHRA), European Heart Journal, 42(35). 3427–3520,
- Jaeggi ET, Silverman ED. The natural history and management of congenital complete atrioventricular block. Cardiology in the Young. 2006;16(1):21–29.
- Brucato A, Cimaz R, Caporali R, Ramoni V, Buyon J. Pregnancy outcomes in patients with autoimmune diseases and anti-Ro/SSA antibodies. Clinical Reviews in Allergy & Immunology. 2011;40(1):27-41.
- Moak JP, Barron KS, Hougen TJ, Wiles HB, Balaji S, Sreeram N, et al. (2001). Congenital heart block: development of late-onset cardiomyopathy, a previously underappreciated sequela. Journal of The American College of Cardiology. 37(1):238-242.