2023: Volume 2, Issue 2
Past Issues
 Abstract
Abstract  PDF
PDFNeonatal Gastric Perforation due to Barotrauma
Sayanthan B1,2,*, Samarakkody U1, Heerthikan K2
1Department of Paediatric Surgery Waikato Hospital New Zealand
2Department of Surgery, Faculty of Medicine, University of Jaffna, Sri Lanka
*Corresponding Author: Dr. Sayanthan Balasubramaniam, Department of Surgery, Faculty of Medicine, University of Jaffna, Sri Lanka; Email: [email protected]
Received Date: July 17, 2023
Publication Date: August 02, 2023
Citation: Sayanthan B, et al. (2023). Neonatal Gastric Perforation due to Barotrauma. Cases. 2(2):13.
Copyright: Sayanthan B, et al. © (2023).
ABSTRACT
Introduction: Gastric perforation in newborns is rare although it is a serious surgical emergency and multiple risk factors contribute to this condition. Clinical Presentation: Here we discuss about a 33 weeks old premature neonate who developed respiratory distress and abdominal distension while on Continuous Positive Airway Pressure. Discussion: Neonatal gastric perforation is seldom seen life-threatening surgical condition commonly seen among premature and low birth weight newborn. The initial first line investigation is abdominal radiological image showing a pneumoperitoneum and it is recommended management that includes early respiratory support, intubation and surgical intervention with broad spectrum antibiotics coverage. Conclusion: Early detection and prompt management improves survival rate and have better prognosis.
Keywords: CPAP, Barotrauma, Positive Pressure Ventilation, Gastric perforation, Neonatology
INTRODUCTION
Gastric perforations in newborns are rare, but serous surgical emergency. Neonatal gastric perforation (NGP) was first described back in early 19th century. Since then the reported numbers has kept increasing, but the mortality has been reducing due to improvement in the neonatal intensive care. The increase in number may be due to the survival of low birth weight and premature newborns. The incidence of NGP is 1 in 5000 live births, accounting for 7% of all neonatal gastrointestinal perforations [1]. Nearly 47% of NGP were considered idiopathic while rest were mainly due to mechanical ventilation, feeding tubes, necrotizing enterocolitis, duodenal/jejunal obstruction, antenatal drugs (aspirin) and oesophageal atresia/trachea oesophageal fistula [2,3]. The symptoms are sudden deterioration of the clinical condition with difficulty breathing and abdominal distension. A simple X-ray of the abdomen is the first line investigation to visualize the pneumoperitoneum. Complete blood count, C - reactive protein, and arterial blood gas will also support investigations in diagnosing the risk factors and future management. The main treatment is ventilatory support and prompt surgical repair of the perforation. This case report is of a case of NGP in a preterm newborn with a single perforation in the greater curvature of the stomach, which was successfully treated with surgery.
CASE PRESENTATION
The baby was delivered by Lower segment Caesarian Section (LSCS) due to fetal distress at the Period of Amenorrhea (POA) of 33 weeks. His birth weight was 1229g and the APGAR score was 6, 9, 10. Bag mask resuscitation was given at birth and kept on Continuous Positive Airway Pressure (CPAP) ventilation with 6cm H2O. The baby tolerated the CPAP for four days. He had an orogastric tube for feeding, and after each feeding tube was clamped to prevent the return of the milk. On the fifth day, he suddenly developed respiratory distress with massive distention of the abdomen. CPAP was not helpful and intubated to secure the ventilation. An urgent abdominal X-ray was done as gastric perforation was suspected. Abdominal X-ray revealed free gas in the peritoneal cavity (Figure 1). The orogastric tube was kept open and aspirated to empty the stomach. Initial blood investigations suggested no evidence of sepsis.
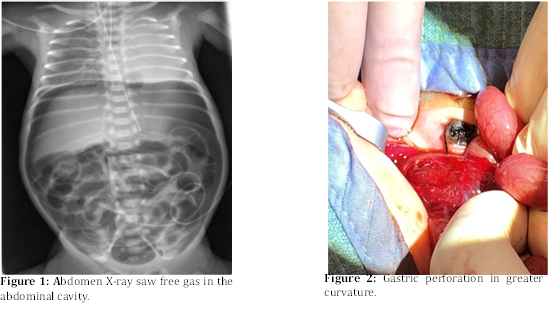
After initial stabilization, explorative laparotomy was performed within 2 hours of the initial suspicion of gastric perforation. Left upper transverse incision used to enter the abdominal cavity. Surgery revealed a 3.5cm linear perforation in the greater curvature of the stomach (Figure 2). Perforation was repaired with absorbable interrupted sutures in double layer. The baby was continuously kept intubated and post-operative recovery was eventful. Ventilation weaned off subsequently on the third day and the baby was discharged after 52 days with no complication.
DISCUSSION
We are reporting a case of NGP in a newborn with risk factors such as prematurity, low birth weight and usage of CPAP. The clinical manifestation of neonatal gastric perforation includes abdominal distention, feeding intolerance, respiratory distress, poor activity, gastrointestinal bleeding, abdominal erythema, and hemodynamic changes as shock [4,5]. This case study noticed a sudden onset of respiratory distress and abdominal distension in a baby on CPAP, mainly indicating gastric perforation due to barotrauma. There were various studies also had mentioned the male gender, prematurity, metabolic acidosis, low birth weight, and hyponatremia as poor prognostic factors. Though some of them had no statistical significance, they were associated with relatively higher mortality rate [6-8]. The team managed the Post perforation period promptly, so this baby didn’t suffer from metabolic acidosis or electrolyte imbalance.
It is believed that a thin gastric wall, due to prematurity, is the reason for NGP. The circular muscle layer of the newborn stomach usually contains multiple gaps, most prominently in the fundus, near the greater curvature. Our case also had the perforation in the greater curvature [7]. Though CPAPs are crucial in severe respiratory conditions it is also associated with a small risk of precipitating gastric perforation. Based on the literature, it is recommended to use a pressure of 6 cm H2O to minimize the occurrence of perforation. Considering the impact of prematurity, further research should be conducted in this aspect. Immediate surgical exploration and correction is necessary once the diagnosis is confirmed. Gastric decompression with NG or OG tube is a recommended practice and be beneficial in initial stabilization and reducing the respiratory distress as it eases diaphragmatic function. With or without omental patch, gastrographic is usually employed to correct the defect while immediate surgery and meticulous post-surgical care are the key factors for favorable outcomes.
CONCLUSION
Gastric perforation should be the first differential diagnosis of a premature neonate on CPAP ventilation without a continuous venting tube in the stomach when it presents with acute onset of abdominal distension and pneumoperitoneum. Early diagnosis and appropriate management contributed to the favorable outcome of this case.
ACKNOWLEDGMENTS
The authors wish to thank, S.Thiruvarangan, Research Assistant who assisted to this piece of research paper preparation and submission process in the final stage of this article.
DISCLOSURE OF CONFLICT OF INTEREST
There is no conflict of interest between the authors as everybody is aware of the work and participated actively
SOURCES OF FUNDING
None
ETHICAL APPROVAL
N/A
STATEMENT OF INFORMED CONSENT
Written informed consent was obtained from the parents of the patient for publication of this case report and accompanying images.
REFERENCES
Aydin M, Deveci U, Taskin E, Bakal U, Kilic M. (2015). Percutaneous peritoneal drainage in isolated neonatal gastric perforation. World J Gastroenterol. 21:12987-12988.
Iacusso C, Boscarelli A, Fusaro F, Bagolan P, Morini F. (2018). Pathogenetic and Prognostic Factors for Neonatal Gastric Perforation: Personal Experience and Systematic Review of the Literature. Front Pediatr. 6:61.
Duran R, Inan M, Vatansever U, Alada? N, Acuna? B. (2007). Etiology of neonatal gastric perforations: Review of 10 years’ experience. Pediatr Int. 49(5):626-630.
Lin CM, Lee HC, Kao HA, Hung HY, Hsu CH, Yeung CY, et al. (2008). Neonatal Gastric Perforation: Report of 15 Cases and Review of the Literature. Pediatr Neonatol. 49(3):65-70.
Garge SS, Paliwal G. (2020). Neonatal Gastric Perforation: Our Experience and Important Preoperative and Intraoperative Caveats to Prognosticate and Improve Survival. J Indian Assoc Pediatr Surg. 25(4):201-205.
Chung MT, Kuo CY, Wang JW, Hsieh WS, Huang CB, Lin JN. (1994). Gastric perforation in the neonate: clinical analysis of 12 cases. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 35(5):460-465.
Chen TY, Liu HK, Yang MC, Yang YN, Ko PJ, Su YT, et al. (2018). Neonatal gastric perforation: a report of two cases and a systematic review. Medicine (Baltimore). 97(17):e0369.
Byun J, Kim HY, Noh SY, Kim SH, Jung SE, Lee SC, et al. (2014). Neonatal gastric perforation: A single center experience. World J Gastrointest Surg. 6(8):151-155.