2022: Volume 1, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFHyperhomocysteinemia and Risk Factors of Metabolic Syndrome in Obese Children
Touzani Asmae1,3*, Mirande Candito2, Ahmed Gaouzi1, Layachi Chabraoui3
1Children’s Hospital, Rabat, Morocco
2Laboratory of Biochemistry, Pasteur Hospital, Nice-France
3Laboratory of Biochemistry and Biology Molecular, Mohamed V University Faculty of Medicine and Pharmacy in Rabat, Morocco
*Corresponding author: Touzani Asmae, Children’s Hospital, Rabat, Morocco. Email: [email protected]
Received: November 25, 2022 Published: December 05, 2022
Citation: Touzani A, et al. (2022). Hyperhomocysteinemia and Risk Factors of Metabolic Syndrome in Obese Childen. Cases. 1(1):4
Copyright: Touzani A, et al. © (2022).
ABSTRACT
Background and Aims: Hyperhomocysteinemia is one of the factors of risk implied in the development of cardiovascular Heart diseases (CHD). Obesity is associated with metabolic anomalies and insulin resistance constituting metabolic syndrome, the aggregate of factors risk of diabetes type 2 and cardiovascular complications. Objectives: The purpose of this work is to determine the levels of serum homocystein in obese children and adolescents and to establish the correlations between homocysteinemia and the components of metabolic syndrome. Patients and methods: The study was carried out on 67 children including 35 obese children (23 Boys, 12 Girls) old of 1 year 8 months at 16 years 4 months (average ± DS: 10.35 ± 3.5 years), with IMC means: 26.5 ± 3.8 kg/m2 and 32 no obese children (12 Boys, 20 Girls) who have an average age of 10 ± 4.6 years, them IMC means is: 16.47 ± 3.28 kg/m2 . The serum lipids are assessed by the enzymatic method, the levels of serum homocystein is determined by HPLC, the insulinemia is determined by technique ELISA. Index of insulin resistance HOMA and the cell ß function (Fc.ß) were calculated according to a formula using the glycemia and the insulinemia. Results: The homocysteinemia high in the obese children is significantly compared with that found in no obese children of the same age (10.6 ± 2.9 vs 7.2 ± 1.3 μmol/l, p12 μmol/l. In our present study, we noticed significantly higher, serum levels average of total cholesterol, LDL cholesterol and triglycerides (P<0,001) in obese children compared to found in no obese or healthy children. There is a significant increase in the rate of uric acid, insulinemia index of insulin resistance (HOMA-IR) (P<0,001) and Fc.ß (P<0,001), reflection of the hepatic insulin resistance. The serum homocystein levels correlate with body mass index (BMI), systolic blood pressure and in particular with uric acid levels. Conclusion: Hyperhomocysteinemia can be associated with metabolic syndrome and varies independently of the components of metabolic syndrome and other factors of risk early stage of the arterial attack. Thus, hyperhomocysteinemia is a predictive marker the development cardiovascular heart disease in obese youths.
Keywords: Obesity, Homocysteinemia, Metabolic syndrome
INTRODUCTION
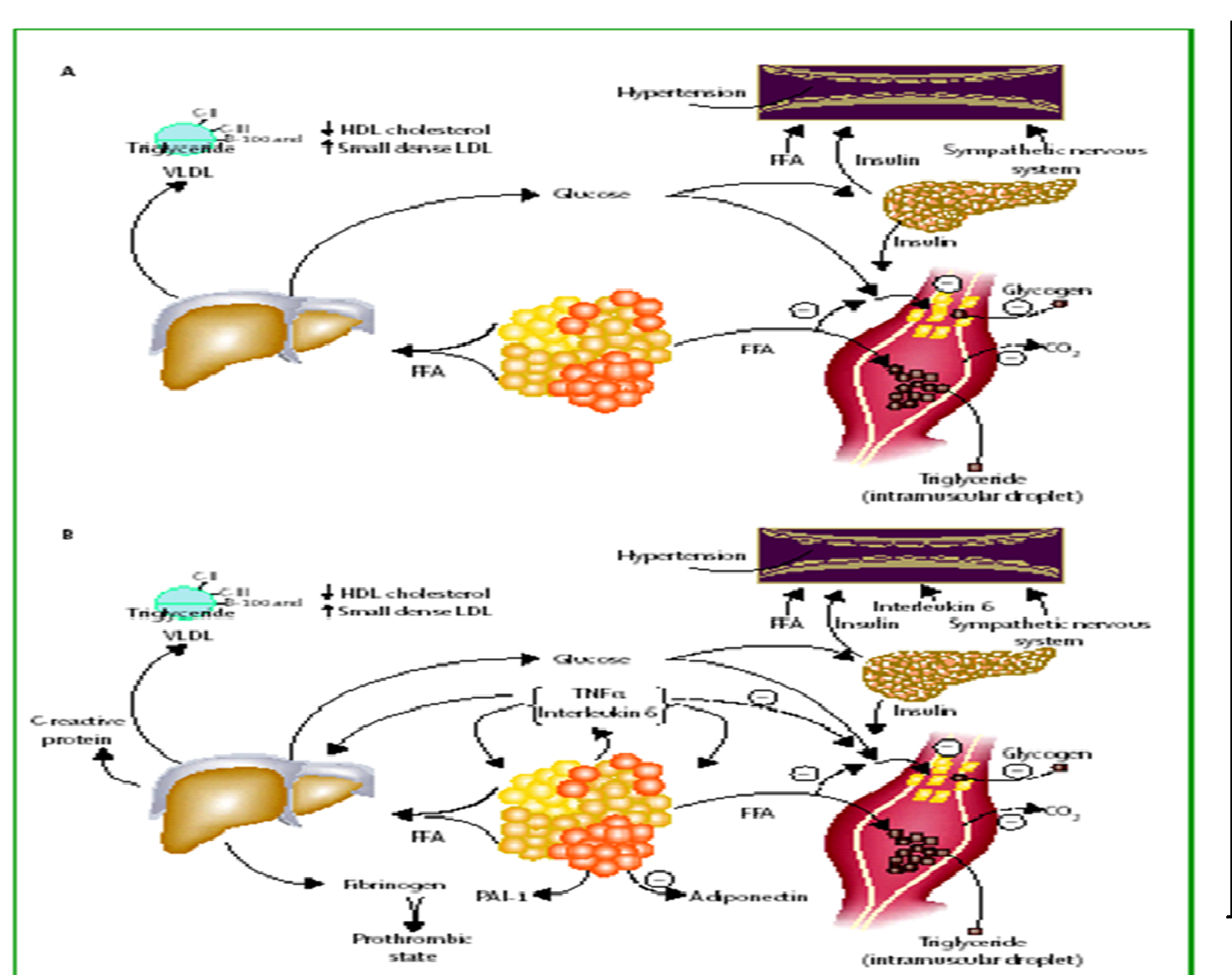
Hyperhomocysteinemia is a risk factor involved in development of cardiovascular disease (CVD). Obesity is associated with metabolic abnormalities (hypertriglyceridemia, hypoHDLémie), abdominal obesity, hypertension, hyperinsulinemia and insulin resistance constitute the metabolic syndrome cluster of risk factors for type 2 diabetes and cardiovascular complications.
In vitro studies provide arguments in favor of the toxicity of excess homocysteine vascular on the wall. Hyperhomocysteinemia contributes to the development of atherosclerosis in obese children.
OBJECTIVES
This work aims to:
• Determine the rate of serum homocysteine in obese children
• Establish correlations between homocysteinemia and risk factors of metabolic syndrome.
Physiopathology of Metabolic syndrome
PATIENTS AND METHODS
The study covers 67 children: 35 obese children (23G, 12 F) aged 1.8 years to 16.4 years (mean ± SD: 10.35 ± 3.5 years) with a mean BMI of 26.5 ± 3.8 kg/m2 .
32 (12G, 20F) children who have witnessed an average age of 10 ± 4.6 years and mean BMI was 16.47 ± 3.28 kg/m2 .
Serum lipid parameters were determined by the enzymatic method.
Serum homocysteine was determined by HPLC. Insulin was assayed by ELISA. The insulin resistance index HOMA and the function of liver cells (Fc.ß) were calculated using a formula:
IR-HOMA = (fasting insulin x fasting glucose) / 22.5
Fc.ß = 20 x fasting insulin / fasting glucose - 3.5
RESULTS
Our results show that homocysteinemia is significantly elevated in obese children compared to that found in children age-matched controls (10.6 ± 2.9 vs 7.2 ± 1.3 mmol/L, P12 µmol / l. Note that there's a non-significant increase in the average serum total cholesterol (1.70 ± 0.34 g / l vs. 1.61 ± 0.31 g / l).
There is a significant elevation of mean concentrations of serum CLDL (1.18 ± 0.21 g / l vs. 0.32 ± 1 g / l) (P <0.05) and triglycerides (1.04 ± 0.74 g / l vs. 0.66 ± 0.25 g / l) (P <0.01) in obese children compared to controls. There's a significant increase in uric acid (36.5 ± 8.7 mg / l vs. 25.9 ± 4.3 mg / l, P <0.001), insulin (10.6 ± 6.3 vs 5.4 ± 3.5 mU / l, P <0.001), index of insulin resistance (HOMA-IR) (0.42 ± 0.27 vs. 0.22 ± 0.14 (P <0.001) and Fc.ß (230, 3 ± 141.9 vs. 118.9 ± 0.3 (P <0.001), reflecting hepatic insulin resistance.
The homocysteine was significantly correlated with systolic blood pressure (r = 0.36, p <0.05) and particularly with uric acid (r = 0.41, P <0.05).

Figure 1: Comparison of parameters Lipids profile and Insulin Resistance Index between obese and controls
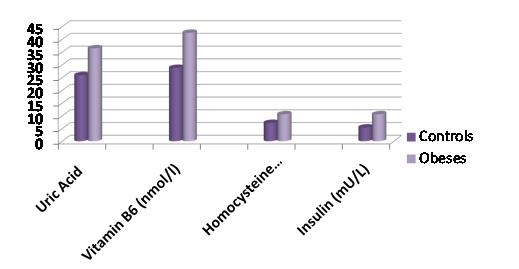
Figure 2: Comparison of parameters of uric Acid, Vitamin B6, Homocystein and Insulin between obese and controls
DISCUSSION
Our results show elevated levels of homocysteine (47%) in obese children compared with healthy children of similar age. Similar results were observed by other authors [5,6]. There is no significant difference between the rate of homocysteine in obese children and witnesses [7].
Our children are obese have a higher rate of total cholesterol, triglycerides, and apoB CLDL. Other authors have shown similar results [8]. Among our 6% obese children with metabolic syndrome defined according to criteria defined by NHANES-ATPIII [9].
Hyperhomocysteinemia is associated with increased waist circumference, triglyceride levels, a lower rate of CHDL, increased uric acid, apoB, hyperinsulinemia and insulin resistance (HOMA-IR). Increasing the Fc.ß shows that there's hepatic insulin resistance in obese children.
Recently, a study described the existence of a metabolic syndrome in patients with four abnormal parameters (waist circumference, systolic or diastolic blood pressure, blood sugar, uric acid, insulin, leptin, triglycerides and CHDL). Some work has shown the elevation of metabolic syndrome varies with the increase in insulin resistance in hyperhomocysteinemia may be associated with the metabolic syndrome.
There continues the relationship between the rate of homocysteine and uric acid. This suggests a decrease in renal elimination. It is not correlated with other components of metabolic syndrome. This result was also confirmed by other authors.
CONCLUSION
Hyperhomocysteinemia may be associated with metabolic syndrome and varies independently of other risk factors.
Hyperhomocysteinemia may be a marker for the development of CVD in obese children.
CONFLICT OF INTEREST
No conflict of interest declared.
ACKNOWLEDGMENTS
I gratefully acknowledge all the authors who contribute to the realization of this research work.
REFERENCES
1. Vanhala M, Vanhala P, Kumpusalo E, Halonen P, Takala J. (1998). Relation between obesity from childhood to adulthood and the metabolic syndrome: population based study. BMJ. 317(7154):319.
2. Kane A, Ly M, Sarr M, Diouf ND, Dia AA, et al. (1998). [Arterial pressure and body mass index of children and adolescents in a rural area of Thiadiaye, Senegal] Dakar Med. 43(1):83-89.
3. Nègre SA. (2001). Homocystéine et athérogénicité des LDL oxydées. Annales de Biologie Clinique. 59:339-353.
4. Fonseca VA, Mudaliar S, Schmidt B, Fink LM, Kern PA, Henry RR. (1998). Plasma homocysteine concentrations are regulated by acute hyperinsulinemia in nondiabetic but not type 2 diabetic subjects. Metabolism. 47(6):686- 689.
5. Gallistl S, Sudi Kilomètre, Erwa W, Aigner R, Borkenstein M. (2001). Determinants of homocysteine during weight reduction in obese children and adolescents. Metabolism. 50(10):1220-1223.
6. Narin F, Atabek JE, Karakukcu M, Narin N, Kurtoglu S, Gumus H, et al. (2005). The association of plasma homocysteine levels with serum leptin and apolipoprotein B levels in childhood obesity. Ann Saudi Med. 25(3):209-214.
7. Martos R, Valle.M, Morales R, Canete R, Gavilan MI, Sanchez-Margalet V. (2006). Hyperhomocysteinemia correlates with insulin resistance and low-grade systemic inflammation in obese prepubertal children. Metabolism. 55(1):72-77.
8. Huang XM, Zhang YY, Yu ZS, Zhu WH, Fu JF, Il J. (2005). Early arterial atherosclerosis and level of plasma homocysteine in simply obese children. Zhonghua Heu Ke Za Zhi. 43(3):192-195.
9. Lyoussi B, Gaouzi A, Bahaymed H, Balafrej A, Chabraoui L. (2006). Complications métaboliques chez les enfants et les adolescents obèses. Fréquence du syndrome métabolique. Diabetes & Metabolism. Abstract No. 31, 88. The Annual Meeting of the ALFEDIAM, March 7-10.